

The integration of basic science with clinical research has led the way for most of the important advances in reconstructive surgery. Investigative research into the mysteries of how the body functions leads to greater understanding of the interdependency of all medical disciplines, and thus contributes to all surgical progress. This is certainly true for plastic and reconstructive surgery as it interacts with and influences other surgical fields. One example is how Nobel Laureate Joseph Murray, M.D., performed the first kidney transplant and-through his plastic surgery expertise-opened up the filed of transplantation surgery.
The research program at University Plastic Surgeons Center for Reconstructive Surgery has a distinguished reputation throughout the country. Our faculty, post-doctoral fellows and medical students are closely involved with many varied basic science disciplines and surgical specialties. Working together, we are meeting our common challenges and finding solutions for shared problems
In the 21st century, our areas of focused research include new microsurgical methods to more safely transplant a wider variety of tissue; new and improved wound treatment; and the development of artificial bone and skin. We are also exploring birth defects-why they occur and how to effectively treat them. With continued research and resultant surgical advances, we can treat individuals even before they are born-in utero-and help them enter the world with an enhanced ability, not only to survive, but to thrive.
Resident and Faculty Research Publications
2016
Yao CA, Swanson J, McCullough M, Taro TB, Gutierrez R, Bradshaw A, Campbell A, Magee WP Jr, Magee WP 3rd. The Medical Mission and Modern Core Competency Training: A 10-Year Follow-Up of Resident Experiences in Global Plastic Surgery. Plast Reconstr Surg. 2016 Sep;138(3):531e-8e. PMID: 27556629
Bhatia A, O'Brien K, Chen M, Wong A, Garner W, Woodley DT, Li W. Dual therapeutic functions of F-5 fragment in burn wounds: preventing wound progression and promoting wound healing in pigs. Mol Ther Methods Clin Dev. 2016Jun 22;3:16041. PMID 27382602
Lee GK, Perrault DP, Bouz A, Patel KM, Hong YK, Wong AK. Surgical Treatment Modalites for Lymphedema. Journal of Aesthetic and Reconstructive Surgery. Vol. 2 No. 2:13, 2016.
Manrique O, Leland HA, Langevin CJ, Wong AK, Carey JN, Patel KM. Optimizing Outcomes Following Total and Subtotal Tongue Reconstruction: A Systematic Review of Contemporary Literature. J Reconstr Microsurg. 2016 Oct 31. [Epub ahead of print] PMID: 27798948
Burtt KE, Rounds AD, Leland HA, Alluri RK, Patel KM, Carey JN. Patient and Surgical Factors Contributing to Postoperative Soft Tissue Infection in Complex Lower Extremity Trauma. Am Surg. 2016 Oct;82(10):940-943. PMID 27779978
Christian D, Leland HA, Rubayi S. Major Repair for End Stage Pressure Ulcer in a Spinal Cord Injury Patient by Disarticulation and Total Thigh Flap: A Case Report. J Derm Plastic Surg. Accepted, pending publication
Johnson MB, Wong AK. Integra-based Reconstruction of Large Scalp Wounds: A Case Report and Systematic Review of the Literature. Plast Reconstr Surg Glob Open. 2016 Oct 24;4(10):e1074. PMID 27826471
Leland HA, Kulber DA. Abdominal Bulge after Retroperitoneal Dissection: The Definitive Management of Repair Using Bone Anchored Reinforced Mesh. Ann of Plast Surg. 2016 May;76 Suppl 3:200-4. PMID: 26954735
Alluri R, Lin C, Iorio M, Leland H, Wong J, Patel K. Vascularized Bone Grafting in Scaphoid Nonunion: A Review of Patient-Centered Outcomes. HAND. 2016 Apr; Epub.
Hong M, Jung E, Yang S, Jung W, Seong YJ, Park E, Bramos A, Kim KE, Lee S, Daghlian G, Seo JI, Choi I, Choi IS, Koh CJ, Kobielak A, Ying QL, Johnson M, Gardner D, Wong AK, Choi D, Hong YK. Efficient Assessment of Developmental, Surgical and Pathological Lymphangiogenesis Using a Lymphatic Reporter Mouse and Its Embryonic Stem Cells. PLoS One. 2016 Jun 9; 11(6): e0157126. PMID: 27280889
Choi D, Ramu S, Park E, Jung E, Yang S, Jung W, Choi I, Lee S, Kim KE, Seong YJ, Hong M, Daghlian G, Kim D, Shin E, Seo JI, Khatchadourian V, Zou M, Li W, De Filippo R, Kokorowski P, Chang A, Kim S, Bertoni A, Furlanetto TW, Shin S, Li M, Chen Y, Wong A, Koh C, Geliebter J, Hong YK. Aberrarnt Activation of Notch Signaling inhibits PROX1 Activity to Enhance the Malignant Behavior of Thyroid Cancer cells. Cancer Res. 2016 Feb 1;76(3):582-93. PMID: 26609053
Thomas DM, Wieck MM, Grant CN, Dossa A, Nowicki D, Stanley P, Zeinati C, Howell LK, Anselmo DM. Doxycycline Sclerotherapy is Superior in the Treatment of Pediatric Lymphatic Malformations. J Vasc Interv Radiol. 2016 Oct 21. pii: S1051-0443(16)30472-9. [Epub ahead of print] PMID: 27776983
Taro T, Yao C, Ly S, Wipfli H, Magee K, Vanderburg R, Magee W 3rd. The Global Surgery Partnership: An Innovative Partnership for Education, Research, and Service. Acad Med. 2016 Jan;91(1):75-8 PMID: 26287915
Christian D, Leland HA, Osias W, Eberlin S, Howell L. Delayed Presentation of a Chronic Morel-Lavallee Lesion. J Radiol Case Rep. 2016 Jul 31;10(7):30-39. PMID: 27761187
Wieck MM, Nowicki D, Schall KA, Zeinati C, Howell LK, Anselmo M. Management of Pediatric Intramuscular venous malformations J Pediatr Surg. 2016 Sep 1. pii: S0022-3468(16)30295-0. [Epub ahead of print] PMID 27622586
McCullough M, Burg M, Lin E, Peng D, Garner W. Steven Johnson Syndrome and Toxic Epidermal Necrolysis in a burn unit: A 15-year experience. Burns. 2016 Aug 20. pii: S0305-4179(16)30243-1. [Epub ahead of print] PMID: 27554629
Alluri RK, Leland HA, Heckmann N. Surgical Research Using National Databases. Ann Transl Med. 2016 Oct;4(20):393.
Macias LH, Kwon E, Gould DJ, Spring MA, Stevens WG. Decrease in Seroma Rate After Adopting Progressive Tension Sutures Without Drains: A Single Surgery Center Experience of 451 Abdominoplasties Over 7 Years. Aesthet Surg J. 2016 Oct;36(9):1029-35. PMID: 26977072
Hoang D, Lin AC, Essilfie A, Minneti M, Kuschner S, Carey J, Ghiassi A. Evaluation of Percutaneous First Annular Pulley Release: Efficacy and Complications in a Perfused Cadaveric Study. J Hand Surg Am. 2016 Jul;41(7):e165-73. Epub 2016 May 13. PMID:2718095
Hoang D, Orgel MI, Kulber DA. Hand Rejuvenation: A Comprehensive Review of Fat Grafting. J Hand Surg Am. 2016 May;41(5):639-44. Review. PMID: 27113709
Kim J, Ho CH, Lewis KE, Garner WL, Chan RY. Delayed-onset thrombocytopenia in a pediatric burn patient. Am J Hematol. 2016 Sep;91(9):958-60. PMID: 27273313
Hoang D, Chen V, Saber S, Patel K, Carey, J. Bilateral Pedicled Superficial Inferior Epigastric Artery Flap in the Treatment of Hidradenitis Suppurativa. Plast Reconstr Surg Glob Open. 2016 Aug 15;4(8):e833 PMID 27622101
Yao CA, Taro TB, Wipfli HL, Ly S, Gillenwater JT, Costa MA, Gutierrez RD, Magee W 3rd. The Tsao Fellowship in Global Health: A Model for International Fellowships in a Surgery Residency. J Craniofac Surg. 2016 Mar;27(2):282-5 PMID: 26963297
Ho AL, Lyonel Carre A, Patel KM. Oncologic reconstruction: General principles and techniques. J Surg Oncol.2016 Jun;113(8):852-64. PMID: 26939879
Yao CA, Magee WP 3rd, Chai G. Reply: Presurgical Nasoalveolar Molding for Cleft Lip and Palate: The Application of Digitally Designed Molds. Plast Reconstr Surg. 2016 May;137(5):904e-5e. PMID: 26783646
El-Sabawi B, Carey JN, Hagopian TM, Sbitany H, Patel KM. Radiation and breast reconstruction: Algorithmic approach and evidence-based outcomes. J Surg Oncol. 2016 Jun;113(8):906-12. PMID: 26750435
Hoang D, Reznik R, Orgel M, Li Q, Mirhadi A, Kulber DA. Surgical Excision and Adjuvant Brachytherapy Versus External Beam Radiation for the Effective Treatment of Keloids: 10-Year Institutional Retrospective Analysis. Aesthetic Surgery Journal. 2016
Morrison, S.D., Chong H.J., Dy, G.W., Grant, D.W., Wilsong, S.C., Brower, J.P., Vedder, N.B., Berli, J.U., Friedrich, J.B., Burretta, K.J., Dreifuss, S.E., Emelife, P.I., Hamilton, K.L., Lo, D.D., Nauta, A.C., Oh, C., Pfaff, M.J., Phillips, N.A., Smith, J.R., Sorkin, M., Suszynski, T.M., Vyas, K.S., Wang, E.D., Wolfswinkel, E.M. Educational Exposure to Transgender Patient Care in Plastic Surgery Training. Plast Reconstr Surg. 2016 Oct; 138(4):944-53.PMID: 27307319
McCullough, M., Wolfswinkel E.M., Magee, W., Ectropion in Facial Tissue Expansion in the Pediatric Population: Incidence, Risk Factors and Treatment Options. Annals of Plastic Surgery. Ann Plast Surg. 2016 Aug 13. [Epub ahead of print] PMID: 27529153
Lee YS, Hsu T, Chiu WC, Sarkozy H, Kulber DA, Choi A, Kim EW, Benya PD, Tuan TL. Keloid-derived, plasma/fibrin-based skin equivalents generate de novo dermal and epidermal pathology of keloid fibrosis in a mouse model. Wound Repair Regen. 2016 Mar;24(2):302-16. PMID: 26683740
Bramos A, Perrault D, Yang S, Jung E, Hong YK, Wong AK. Prevention of Postsurgical Lymphedema by 9-cis Retinoic Acid. Ann Surg. 2016 Aug;264(2):353-61. PMID: 26655920
Macias LH, Stevens WG. Commentary on: An Assessment of Gender Differences in Plastic Surgery Marketing in the United States: Are We Neglecting Our Male Patients?Aesthet Surg J. 2016 Jan;36(1):111-2. PMID: 26609142
2015
Wong AK, Nguyen TJ, Peric M, Shahabi A, Vidar EN, Hwang BH, Niknam LS, Chan LS, Urata MM. Analysis of risk factors associated with microvascular free flap failure using a multi-institutional database. Microsurgery. 2015 Jan;35(1):6-12. PMID: 24431159
Chai G, Tan A, Yao CA, Magee WP 3rd, Junjun P, Zhu M, Bogari M, Hsu Y, Xu H, Zhang Y. Treating Parry-Romberg Syndrome Using Three-Dimensional Scanning and Printing and the Anterolateral Thigh Dermal Adipofascial Flap. J Craniofac Surg. 2015 Sep;26(6):1826-9. PMID 26355969
Bartsich S, Yao CA. Is frosting effective? The role of retention sutures in posttraumatic orbital reconstruction surgery. J Plast Reconstr Aesthet Surg. 2015 Dec;68(12):1683-6. PMID 26319057
Shen C, Yao CA, Magee W 3rd, Chai G, Zhang Y. Presurgical nasoalveolar molding for cleft lip and palate: the application of digitally designed molds. Plast Reconstr Surg. 2015 Jun;135(6):1007e-1015e. PMID 26017607
Ma J, Huang YQ, Yao C, Ma SQ, Meng T, Ma M, Su GH, Zhai K, Zhou ZW, Zhu JF, Shi B. Parental health and social support in the first trimester of pregnancy and the risk of oral clefts: a questionnaire-based, case-control study. Plast Reconstr Surg. 2015 Jan;135(1):212-8 PMID: 25539307
Costa MA, Yao CA, Gillenwater TJ, Taghva GH, Abrishami S, Green TA, Magee WP. Telemedicine in Cleft Care: Reliability and Predictability in Regional and International Practice Settings. J Craniofac Surg. 2015 Jun;26(4):1116-20. PMID 26010103
Leland HA, Alluri RK, Iorio ML, Carey JN, Constantinescu T, Patel KM. Complex Hand and Wrist Reconstruction Using Free Vascularized Bone Grafts. Plast Reconstr Surg. 2015 Oct. 136(4) Suppl:25-6. PMID: 26397515
Leland HA,Kulber DA. Abdominal Bulge after Retroperitoneal Dissection: The Definitive Management of Repair Using Bone Anchored Reinforced Mesh. Plast Reconstr Surg. 2015 Apr:135(4) Suppl:1193. PMID 26954735
Gould DJ, Nadeau MH, Macias LH, Stevens WG. Inverted Nipple Repair Revisited: A 7-Year Experience. Aesthet Surg J. 2015 Feb 12 [Epub ahead of print] PMID 25681105. Award: Best Resident Clinical Paper 2015 by ASJ.
Nadeau MH, Gould DJ, Macias LH, Spring MA, Stevens WG. Superior pedicle technique of reduction mammaplasty: a stepwise approach. Aesthet Surg J. 2015 Jan;35(1):94-104. PMID 25568240
Hagopian TM (2015). The University of Southern California Intern Handbook: First Edition, 2015. Los Angeles, California: University of Southern California, Keck School of Medicine, Department of Surgery.
P. Rudnick, F. Liang, N. Prince, S. Lipsitz, J. May, L. Guo. What Made Them Successful: An Introspective Survey of AAPS Members.Plast Reconstr Surg Global Open. 2015 Apr 7;3(3):e327 PMID 25878938
F. Liang, P. Rudnick, N. Prince, S. Lipsitz, J. May, L. Guo. An Evaluation of Plastic Surgery Resident Selection Factors. Journal of Surgical Education. 2015 Jan; 72(1):8-15. PMID 25218369
Solanky D, Hwang SM, Stone G, Gillenwater J, Carey JN. Successful Surgical Treatment of Severe Calciphylaxis Using a Bilayer Dermal Replacement Matrix. Wounds. 2015 Nov;27(11):302-7. Review. PMID: 26574752
Starnes-Roubaud MJ, Peric M, Chowdry F, Nguyen JT, Schooler W, Sherman R, Carey JN. Microsurgical Lower Extremity Reconstruction in the Subacute Period: A Safe Alternative. Plast Reconstr Surg Glob Open. 2015 Aug 10;3(7):e449. PMID: 26301138
Karan A, Amado V, Vitorino P, Kulber D, Taela A, DeUgarte DA. Evaluating the socioeconomic and cultural factors associated with pediatric burn injuries in Maputo, Mozambique. Pediatr Surg Int. 2015 Nov;31(11):1035-40. PMID: 26280740
Carey JN, Minneti M, Leland HA, Demetriades D, Talving P. Perfused fresh cadavers: method for application to surgical simulation. Am J Surg. 2015 Jul;210(1):179-87. PMID: 25890815
Stevens WG. Response to "Cryolipolysis: The Importance of Scientific Evaluation of a New Technique". Aesthet Surg J. 2015 Jul;35(5):NP120-2. PMID: 25846670
Hammoudeh JA, Howell LK, Boutros S, Scott MA, Urata MM. Current Status of Surgical Planning for Orthognathic Surgery: Traditional Methods versus 3D Surgical Planning. Plast Reconstr Surg Glob Open. 2015 Mar 6;3(2):e307. PMID 25750846
Stevens WG, Bachelor EP. Cryolipolysis conformable-surface applicator for nonsurgical fat reduction in lateral thighs. Aesthet Surg J. 2015 Jan;35(1):66-71. PMID: 25568236
Wong AK, Joanna Nguyen T, Peric M, Shahabi A, Vidar EN, Hwang BH, Niknam Leilabadi S, Chan LS, Urata MM. Analysis of risk factors associated with microvascular free flap failure using a multi-institutional database. Microsurgery. 2015 Jan;35(1):6-12. PMID: 24431159
Figueiredo JC, Ly S, Magee KS, Ihenacho U, Baurley JW, Sanchez-Lara PA, Brindopke F, Nguyen TH, Nguyen V, Tangco MI, Giron M, Abrahams T, Jang G, Vu A, Zolfaghari E, Yao CA, Foong A, DeClerk YA, Samet JM, Magee W 3rd. Parental risk factors for oral clefts among Central Africans, Southeast Asians, and Central Americans. Birth Defects Res A Clin Mol Teratol. 2015 Oct;103(10):863-79. PMID: 26466527
Spring MA, Hartmann EC, Stevens WG. Strategies and Challenges in Simultaneous Augmentation Mastopexy. Clin Plast Surg. 2015 Oct;42(4):505-18. PMID: 26408440
Carey JN, Caldwell AM, Coughlin RR, Hansen S. Building Orthopaedic Trauma Capacity: IGOT International SMART Course.J Orthop Trauma. 2015 Oct;29 Suppl 10:S17-9. PMID: 26356207
Chai G, Tan A, Yao CA, Magee WP 3rd, Junjun P, Zhu M, Bogari M, Hsu Y, Xu H, Zhang Y. Treating Parry-Romberg Syndrome Using Three-Dimensional Scanning and Printing and the Anterolateral Thigh Dermal Adipofascial Flap. J Craniofac Surg. 2015 Sep;26(6):1826-9. PMID: 26355969
El-Sabawi B, Sosin M, Carey JN, Nahabedian MY, Patel KM. Breast reconstruction and adjuvant therapy: A systematic review of surgical outcomes. J Surg Oncol. 2015 Oct;112(5):458-64. PMID: 26345465
Chien MC, Mascarenhas L, Hammoudeh JA, Venkatramani R. Zoledronic Acid for the Treatment of Children With Refractory Central Giant Cell Granuloma. J Pediatr Hematol Oncol. 2015 Aug;37(6):e399-401. PMID: 26056788
Shen C, Yao CA, Magee W 3rd, Chai G, Zhang Y. Presurgical nasoalveolar molding for cleft lip and palate: the application of digitally designed molds. Plast Reconstr Surg. 2015 Jun;135(6):1007e-1015e. PMID: 26017607
Fine NA, Lehfeldt M, Gross JE, Downey S, Kind GM, Duda G, Kulber D, Horan R, Ippolito J, Jewell M. SERI surgical scaffold, prospective clinical trial of a silk-derived biological scaffold in two-stage breast reconstruction: 1-year data. Plast Reconstr Surg. 2015 Feb;135(2):339-51. PMID: 25502862
Resident Research Presentations
Is Post-operative Intensive Care Unit Care Necessary Following Cranial Vault Remodeling for Sagittal Synostosis?
Erik M. Wolfswinkel, M.D., Lori K. Howell, M.D., Beina Azadgoli, M.S., Artur Fahradyan, M.D., J. Gordon McComb M.D., Mark M. Urata M.D., D.D.S.
Background: Of US craniofacial and neruosurgeons, 94% routinely admit patients to the intensive care unit (ICU) following cranial vault remodeling (CVR) for correction of sagittal synostosis. This study aims to examine safety and cost of direct ward admission following primary CVR for sagittal synostosis.
Methods: An IRB approved retrospective review was undertaken of all patients who underwent primary CVR for isolated sagittal craniosynostosis over the period of 2009-2015 at a single pediatric hospital. Patient demographics, perioperative course and outcomes were recorded.
Results: 121 patient were identified whom110 patients met inclusion criteria of CVR for isolated sagittal synostosis in the absence of other major medical problems. Average age at operation was 6.7 months with mean follow-up of 19.8 months. Of 110 patients, 98 (89%) were admitted to a general ward for postoperative care while the remaining 12 (11%) were admitted to the ICU for preoperative or perioperative concerns. Among ward admitted patients, there were 4 (3.63%) minor complications, none of which required ICU transfer. Average hospital stay was 3.7 days. Our institution’s financial difference in cost of ICU versus ward bed are $5,520.00 on average per bed/day. Projected health care cost savings of this patient cohort assuming just 1 ICU post-operative day stay would be $540,960.00 with multiples of this amount for additional days.
Discussion: Despite the common practice of ICU care following CVR for sagittal craniosynostosis, this review indicates general ward management is safe and cost effective. It is suggested that post-operative admission to the ICU following CVR for sagittal synostosis be considered on an individual basis with only a small percentage needing a higher level of care.
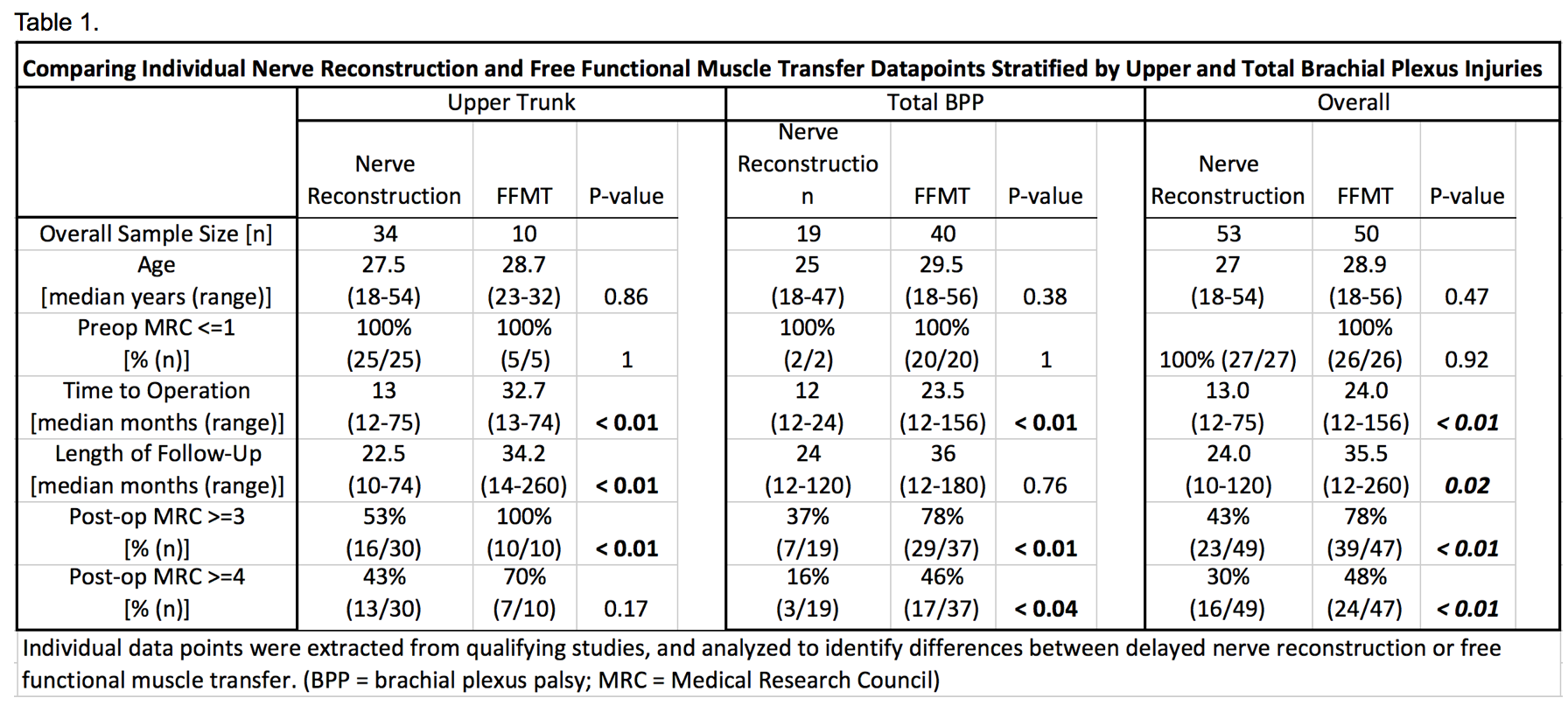
Recovery of Elbow Flexion After Delayed Nerve Reconstruction versus Free Functional Muscle Transfer for Traumatic Brachial Plexus Palsy: A Systematic Review
Don Hoang, MD, MHS, Plastic and Reconstructive Surgery, Keck School of Medicine, University of Southern California, Los Angeles, CA,
Vivi W Chen, BS, Keck School of Medicine, University of Southern California, Los Angeles, CA and
Mitchel Seruya, MD, Plastic Surgery, USC Keck School of Medicine and CHLA, Los Angeles, CA
Purpose: In delayed presentation of brachial plexus trauma, the question arises as to whether donor nerves should be devoted to nerve reconstruction or reserved for free functional muscle transfer (FFMT). The purpose of this study was to systematically review recovery of elbow flexion after delayed nerve reconstruction versus FFMT for traumatic brachial plexus palsy.
Methods: A systematic review was performed using the PUBMED, SCOPUS, and Cochrane databases in order to identify all cases of traumatic brachial plexus palsy in patients 18 years or older. Patients who underwent delayed (>=12 months) nerve reconstruction or FFMT for elbow flexion were included. Demographics were recorded, including age, time to operation, and level of brachial plexus injury. Functional outcomes were evaluated, including British MRC strength and range of motion for elbow flexion.
Results: Thirty-three studies met criteria (Figure 1) for a total of 103 patients (53 delayed nerve reconstruction, 50 FFMT). The methodological quality of included studies (MINORS) ranged from 5092%, with a median MINORS criteria score of 54% (IQR 5471%) for nerve reconstruction and 54% (IQR 5456%) for FFMT articles (p=0.72). Surgical age and preoperative elbow flexion were no different across the groups, whereas time to surgery and followup time were significantly longer in the FFMT group (Table 1). For upper trunk injuries, 53% of nerve reconstruction patients versus 100% of FFMT patients achieved M3 or greater strength (p<0.01) and 43% of nerve reconstruction patients versus 70% of FFMT patients achieved M4 or greater strength (p=0.17). In total brachial plexus injuries, 37% of nerve reconstruction patients versus 78% of FFMT patients achieved M3 or greater strength (p<0.01) and 16% of nerve reconstruction patients versus 46% of FFMT patients achieved M4 or greater strength (p<0.04).
Conclusion: In delayed presentation of traumatic brachial plexus injuries, donor nerves should be reserved for free functional muscle transfer rather than for nerve reconstruction to restore elbow flexion.
Extracranial to Intracranial Flow through Flaps
Azadgoli B, Leland H, Wolfswinkel E, Lanier B, Hoang D, Russin J, Carey J
Introduction: Extracranial-intracranial bypass is indicated in ischemic disease such as moyamoya, certain intracranial aneurysms, and other complex patient conditions. Soft tissue transfer is indicated for craniofacial trauma and tumors and in cases of indirect cerebral revascularization. Fascial, skin, omental, and muscle flaps have been used for these indications. In this report, we present our series of flow through flaps for cerebral revascularization in conjunction with soft tissue reconstruction.
Methods: A retrospective review of a prospectively maintained database was performed. Five patients were identified who required direct arterial bypass in conjunction with a soft tissue procedure for indirect revascularizations or soft tissue reconstruction.
Results: Indications for arterial bypass included intracranial aneurysm (n=1) and moya moya disease (n=4). Indications for soft tissue reconstruction included infected cranioplasty (1) and indirect cerebral revascularization for moya moya disease (4). Flaps included flow through radial forearm fascial flaps (2), a flow through radial forearm fasciocutaneous flap (1) and flow through pedicled temporoparietal fascial flap (2). The superficial temporal vessels (3) and facial vessels (3) were used as the recipient site pedicle. Flow through reperfusion was established into the middle cerebral artery (3) and anterior communicating artery (2). There were no intraoperative complications. All flaps survived and there were no donor site complications. Postoperative imaging demonstrated graft patency in 4/5 patients. In one case of flow through TPF flap, the direct graft failed, but the indirect flap remained vascularized.
Conclusions: Flow through flaps can be safely used for conditions where combined arterial bypass and soft tissue procedures are required. Early outcomes have not demonstrated any major complications. Long-term results with direct and indirect re-vascularization are pending.
Variables Associated with Outcomes in Peripheral Nerve Repair
Azadgoli B, Hoang D, Leland H, Bonsu N, Carey J
Background: Data regarding outcomes after peripheral nerve injuries is limited, and the optimal management strategy for an acute injury is unclear. The aim of this study was to examine specific patient and surgical factors that impact motor and sensory outcomes after peripheral nerve injury.
Methods: This was a single center, retrospective study at a metropolitan level 1 trauma center. Patients with traumatic peripheral nerve injury from 01/2010 – 06/2015 were included. Patients who died, required amputation, suffered brachial plexus injury, or had missing motor-sensory exams were excluded. Motor and sensory exams were graded 0-5 by the Modified British Medical Research Council system. Operative repair of peripheral nerves was analyzed for patient characteristics, anatomic nerve injury, level of injury, associated injuries, days until repair, and repair method.
Results: 311 patients met inclusion criteria. 258 (83%) patients underwent operative management, and 53 (17%) underwent non-operative management. Those who required operative intervention had significantly more penetrating injuries 85.7% vs 64.2% (p<0.001), worse initial motor scores 1.19 vs 2.23 (p=0.004), and worse initial sensory exam scores 1.75 vs 2.28 (p=0.029). Predictors of improved operative motor outcomes on univariate analysis were Injury Severity Score (ISS) <15 (p=0.013), male sex (p=0.006), while upper arm level of injury was a predictor (p=0.041) of poor outcome. Nerve reconstruction type between primary, allograft, autograft, or nerve tube did not influence motor outcomes (p=0.15). Multivariate analysis did not confirm level of nerve injury to be predictive of outcome. Univariate analysis identified distal forearm level of injury (p=0.026) and autograft repair (p=0.048) as predictors of poor sensory outcome. These variables were not found to be significant on multivariate analysis. Days to nerve repair (≤ 24 hours versus >24 hours, p=0.834) did not influence motor-sensory outcome.
Conclusion: Outcomes were primarily influenced by patient characteristics, and injury level to a lesser degree, rather than operative repair characteristics.
Table 1. Outcomes: Motor Recovery and Level Injury
Table 2. Predictors of Improved Motor-Sensory Outcomes: Univariate Analysis
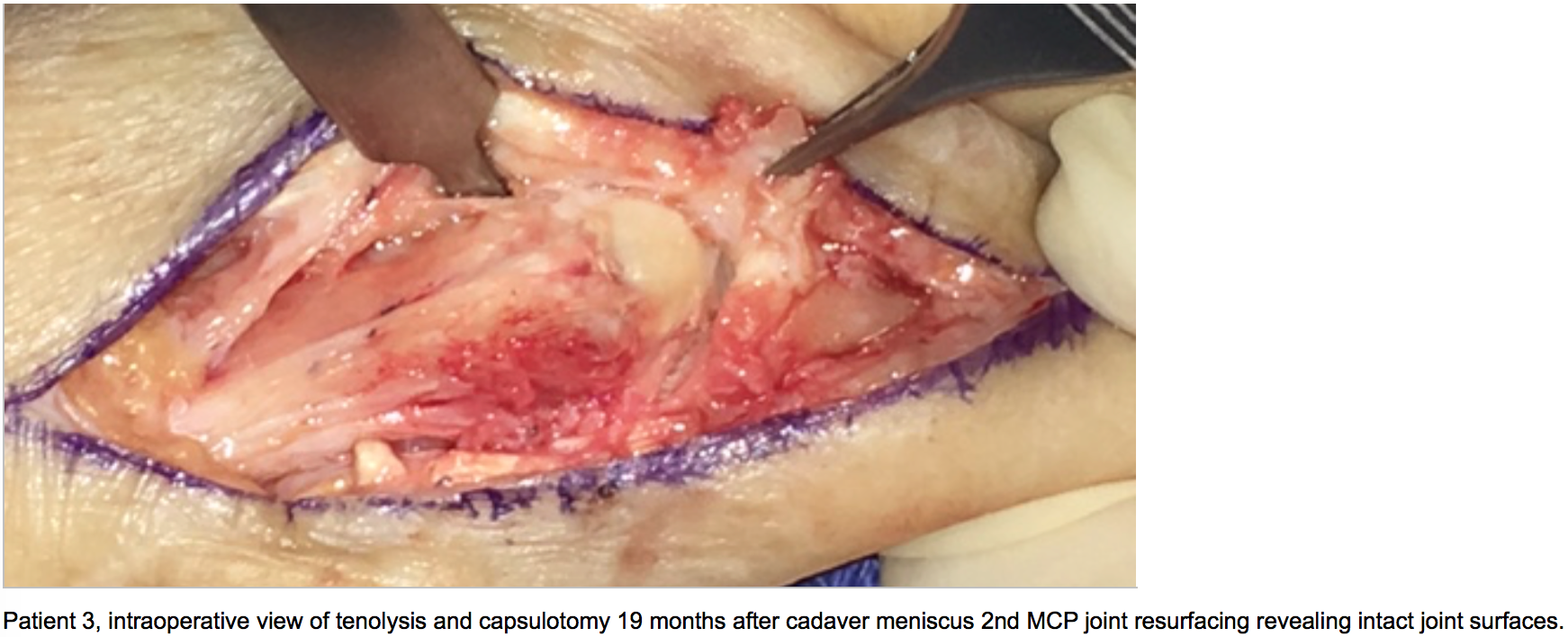
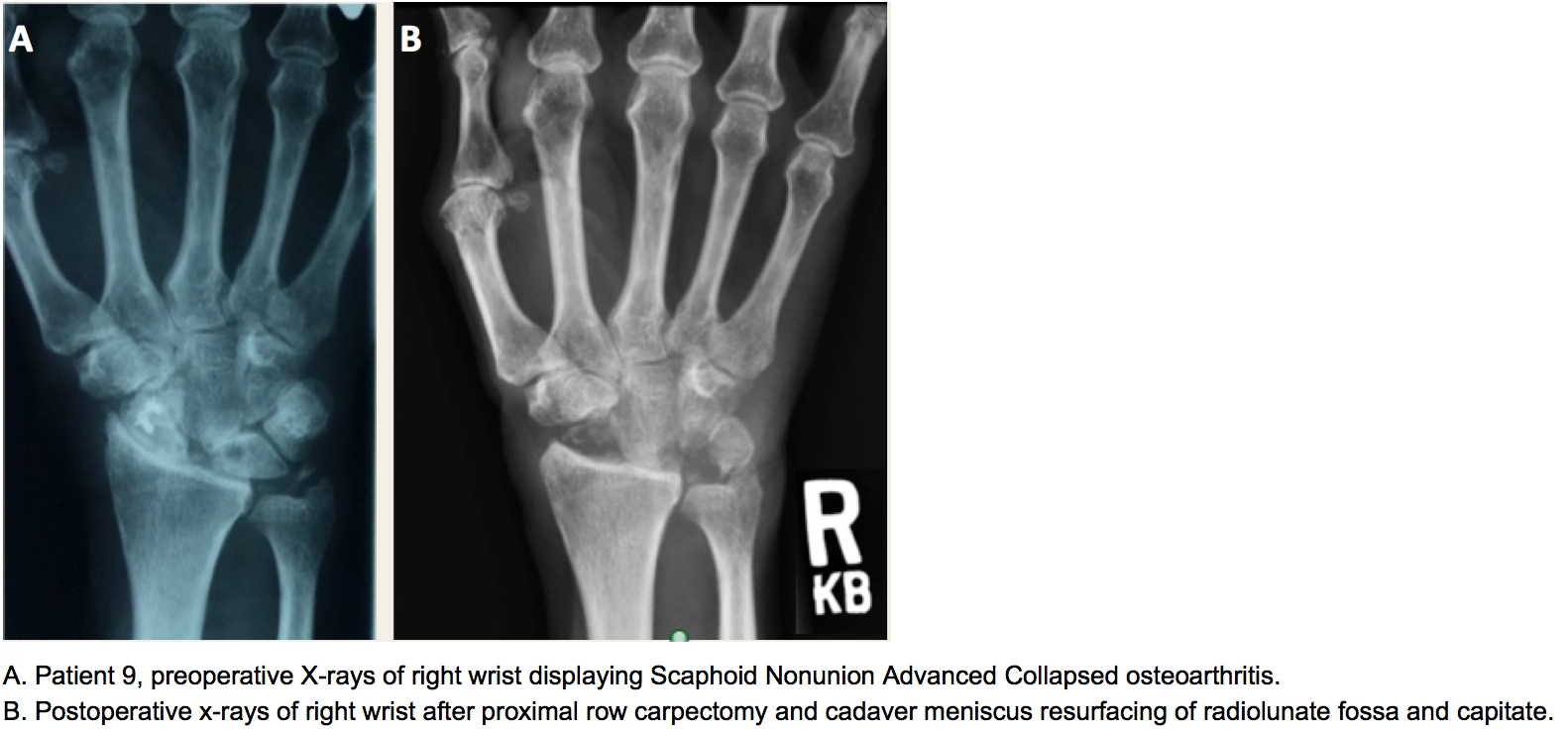
Long Term Successful Wrist and Finger Joint Arthroplasty Using Cadaveric Meniscus for Osteochondral Defects in the Radiocarpal, Metacarpal, and Proximal Interphalangeal Joints
Don Hoang, MD1, Dan Gould, MD PHD1, Matt Orgel, BS1, Myles Cohen, MD2, David A. Kulber, MD2
1Plastic and Reconstructive Surgery, Keck School of Medicine, University of Southern California, Los Angeles, CA
Hypothesis: Osteochondral defects of the radiocarpal, metacarpophalangeal, and proximal-interphalangeal joints often necessitate joint arthrodesis or mechanical arthroplasty, which has a limited lifespan. In severely arthritic wrist and finger joints, we propose a novel adjunct for joint salvage using cadaveric meniscus for joint resurfacing as an off-the-shelf alternative to address osteochondral defects and restore normal intra-articular contact stress.
Methods: Five radiocapitate, five metacarpophalangeal, and three proximal-interphalangeal and one carpometacarpal joints in clinical patients with osteochondral defects received cadaveric meniscus to facilitate arthroplasty. Patient demographic, peri-operative pain, range of motion, complications were examined.
Results: Patients aged 17 to 73 years old (average 54.6 years old) underwent joint reconstruction for scaphoid non-union (n=1), scaphoid-lunate advanced collapse (n=4), or osteoarthritis of MCP/CMC (n=6) or PIP (n=3) joints . Successful arthroplasty with joint space preservation occurred in all joints. Patients underwent postoperative hand therapy at 3 weeks and had significant reduction in pain scale score (average 9.7 to 1.7) and improved range of motion [average degrees flexion 15 (wrist), 46 (MCP), PIP (50); extension 30 (wrist)]. No complications resulted; only a revision tenolysis and capsulotomy were required for PIP and MCP arthroplasties. Post-operative films reveal preservation of arthroplasty joint space after an average 13.7 months follow-up.
Summary Points: We believe that meniscus is a viable joint salvage adjunct to preserve pain-free motion and avoid total joint arthrodesis. We have provided a case series of 14 patients who have benefited from the use of cadaver meniscus in hand joint arthroplasty Cadaveric meniscus advantageously maintains a low metabolic demand, biointegrates, and is surgically malleable.



THE KRUKENBERG PROCEDURE IN THE PEDIATRIC PATIENT: A CASE SERIES
T. JoAnna Nguyen MD1, John Lawrence MD2, Katherine Au MD1
University of Southern California, Keck School of Medicine1 Division of Plastic & Reconstructive Surgery University of California, Los Angeles2 Division of Hand Surgery
BACKGROUND:
The loss of a hand has devastating consequences on one’s functional independence, and reconstruction after hand amputation is limited. The Krukenberg operation, separating the radius and ulna through the interosseous membrane to the level of the pronator teres, provides patients with hand absence a useful and sensate pincer mechanism that is helpful for activities of daily living. Historically, this procedure has been reserved for blind bilateral amputee patients or in areas where prosthetic devices are unavailable. In this series, we present the long-term follow up of pediatric patients who have undergone the Krukenberg procedure.
METHODS: We performed a retrospective chart review of patients who underwent the Krukenberg procedure at a single institution. Patient demographic, pre-operative, operative and post-operative data were examined.
RESULTS: From 1987 to 2013, we identified 7 consecutive pediatric patients who underwent the Krukenberg procedure. Indications for surgery included congenital transverse limb deficiency (n=4) and traumatic amputation (n=3). Average follow up was 4.4 years (range: 2 to 10 years), and all patients (n=7) were male. None of the patients were blind. Complications included skin breakdown (n=2) and heterotopic ossification (n=1). Overall, the patients did well and were able to use the Krukenberg to perform activities of daily living.
CONCLUSION: In this series, we demonstrate the feasibility and safety of performing the Krukenberg procedure in pediatric patients. In certain populations where there are limited resources for prostheses, this procedure offers the patient functional independence with a sensate upper extremity capable of prehension.

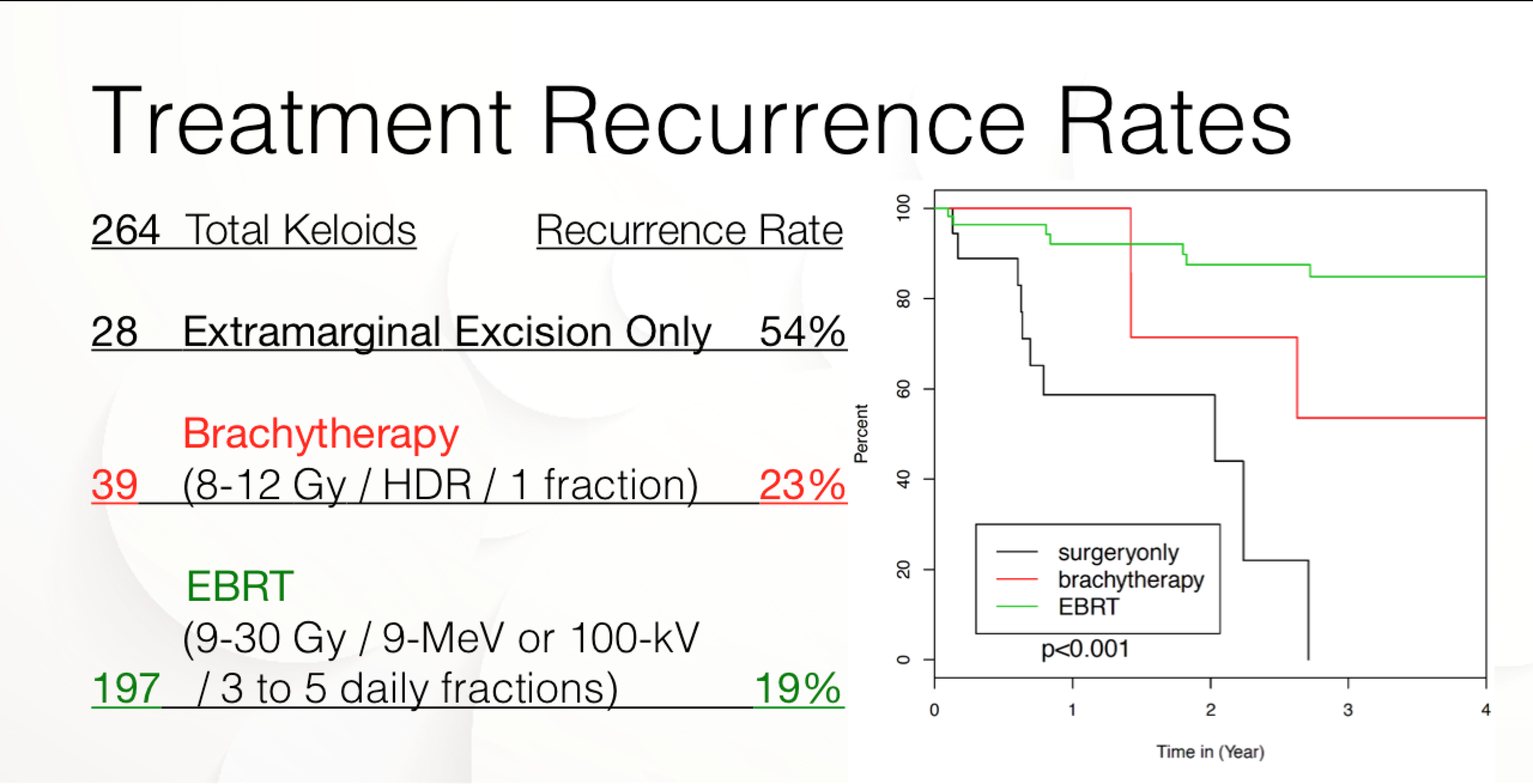
Surgical Excision and Adjuvant Brachytherapy versus Electron Beam Radiation for the Effective Treatment of Keloids – a 10-year Institutional Review
Don Hoang, MD, MHS, Plastic and Reconstructive Surgery, USC Keck School of Medicine, Los Angeles, CA; Robert Reznik, MD, Department of Radiation Oncology, Cedars-Sinai Medical Center, Los Angeles, CA; Matthew Orgel, BS, Plastic and Reconstructive Surgery, USC Keck School of Medicine, Los Angeles, CA, Amin Mirhadi, MD, Department of Radiation Oncology, Cedars-Sinai Medical Center, Los Angeles, CA; and David A. Kulber, MD, Division of Plastic and Reconstructive Surgery, Cedars-Sinai Medical Center, Los Angeles, CA., Plastic and Reconstructive Surgery, USC Keck School of Medicine.
Purpose: Surgically excised keloids recur at reported rates of 45-100%. Radiation therapy is often reserved for the most refractory keloids due to concerns over its sequelae. Electron beam radiation (EBRT) is the most common radiation modality with a reported 17 to 33% recurrence rate. Meanwhile, one case reports that high-dose rate (HDR) brachytherapy has roughly a 10 to 20% recurrence rate. This study aimed to determine whether the adjunct use of brachytherapy or EBRT achieved greater reduction in keloid recurrences compared to excision alone.
Methods: 128 patients with combined 264 keloid lesions were treated by surgical excision alone (n = 28), surgical excision followed within 24 hours by postoperative HDR single-catheter interstitial brachytherapy (Ir-192) totaling 8 to 12 Gy delivered over one fraction (n = 39) or 6- or 9-MeV EBRT totaling 9 to 16 Gy divided over one to three fractions (n = 197).
Results: Of the lesions excised alone, 46% (13/28) recurred; 23% of brachytherapy treated lesions (9/39 with average follow-up 16.5 months) recurred and 21% of EBRT treated lesions recurred (37/197 with average follow-up 54 months). (Table 1) Adjunctive radiation therapy resulted in significant reduction of keloid recurrence (p = 0.01). There was no significant difference in recurrences after brachytherapy versus EBRT modalities (p = 0.53). (Table 1)
Conclusion: Brachytherapy and EBRT significantly reduce keloid recurrences compared to surgical excision alone, but neither appears to hold an advantage over the other in terms of recurrence rates. However, brachytherapy has the potential to reduce the total dosage and fractions of radiation delivered. This warrants further work up with a head to head study.



2016 AAHS Annual Meeting
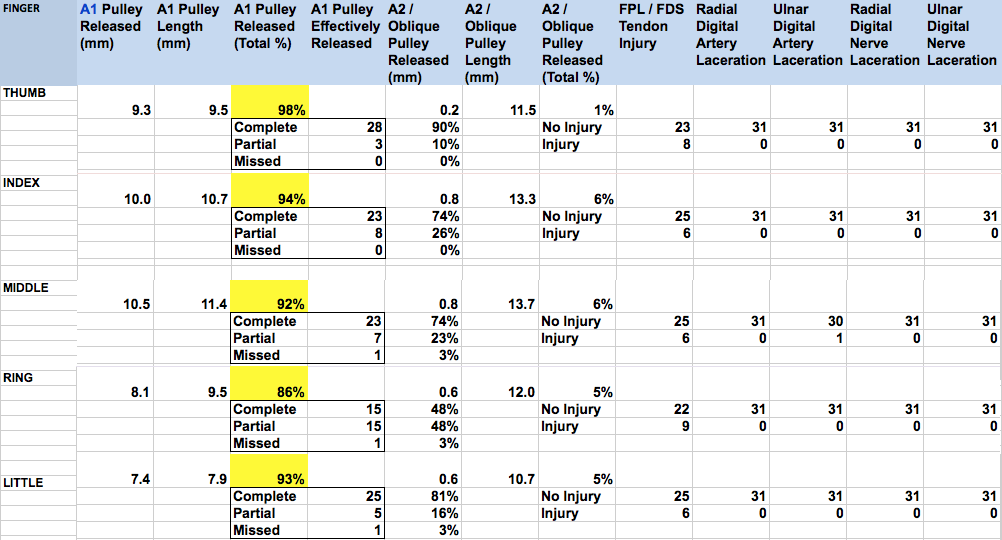
Evaluation of Percutaneous First Annular Pulley Release: Efficacy and Complications in a Perfused Cadaveric Study
Don Hoang, MD, MHS (1), Ann C. Lin, BS (1), Anthony Essilfie, MD (1), Alidad Ghiassi, MD (1), Stuart Kuschner, MD (2) and Joseph Carey, MD (1), (1)Plastic and Reconstructive Surgery, USC Keck School of Medicine, Los Angeles, CA, (2)Hand Surgery, Cedars Sinai Medical Center, Los Angeles, CA
Background: Trigger finger is the most common entrapment tendinopathy, with lifetime-risks of 2-3 percent (diabetics ~10%). Open tenovaginotomy is standard therapy associated with high success rates. Despite percutaneous trigger finger release (PFTR) success rates over 94%, controversy remains over its use due to fear of digital neurovascular injury. This study aimed to assess the safety of blind versus sonographically-guided(US) first annular (A1) pulley releases performed on a perfused cadaveric model (fig.1).
Methods: 155 (124 fingers and 31 thumbs) percutaneous A1 pulley releases were performed on un-embalmed cadavers (65 female, 90 male fingers) with restored perfusion (fig.2) and an 18-gauge needle. 45 fingers and thumbs were completed with US while 110 were completed without US. Each digit was dissected and assessed for A1 pulley release completeness as well as neurovascular, flexor tendon, and A2 pulley injury (fig.3).
Results: Overall, 114 (74%) A1 finger and thumb pulleys were effectively released. There were 38 (24%) partial releases and only three digits were completely missed (2%) (fig.3). Thumbs had 28 complete (90%) and 3 partial releases (10%). Index fingers had 23 complete (74%), and 8 partial releases (26%); long fingers had 23 complete (74%), 3 partial (23%), and 1 missed release (3%); ring fingers had 15 complete (48%), 15 partial (48%), 1 missed release (3%); while little fingers had 25 complete (81%), 5 partial (16%), and 1 missed release (3%) (fig.1). Average percent of A1 pulley length released for all fingers was 93%. No significant flexor tendon injury (partial or complete lacerations) was seen in any digit, although longitudinal scoring was found in 35 fingers (23% overall; total of 9 ring fingers, 8 thumbs, 6 index, 6 middle, 6 little fingers). No digital, radial or ulnar, nerves was found to be injured (fig.5). Only one ulnar middle finger digital artery was lacerated (1%) in a finger with a partial flexion contracture. The ultrasound-guided PTFR technique was not more likely to result in a complete pulley release compared to the blind needle technique (80% versus 72%; P < 0.26).
Conclusion: Both blind and ultrasound-assisted percutaneous releases of the A1 pulley can be performed safely and effectively for all fingers including the thumb. Perfusion of cadaver digits enhances surgical simulation for PTFR training, especially for in-vivo identification of structures by US with doppler-flow. Our cadaveric data support published clinical investigations recommending percutaneous A1 pulley release in the management of trigger finger.




Outcome of Limb preservation after Sarcoma resection, a Retrospective analysis of Clinical Outcomes
CarreAL1, ChattaA1, Bramos T1,ShermanR1, Schooler W1, Carey J1, Menendez LR2, Wong, AK1. Department of Plastic1 and Orthopaedic surgery2, University of Southern California, Keck School of Medicine, Los Angeles California
Purpose: Oncologic surgical management of upper and lower extremity sarcoma with limb sparing procedures and adjuvant radiation therapy results in complex wound defects. The rate of wound complications after primary closure is significant. Early interventions by plastic surgeons may prevent and/or limit wound related morbidity. We hypothesize that wound outcomes are influenced by wound size and early involvement of plastic surgery. We believe early aggressive reconstructive approaches and appropriate wound management can minimize wound complications.
Method: We performed a retrospective analysis of patients from a single oncologic surgeon and a team of reconstructive surgeons at the University of Southern California (USC)- Keck School of medicine. Over a 5-year period, April 2009- August 2014 we identified patients that underwent resection of bone or soft tissue sarcoma of the upper or lower limb. 160 patients met the inclusion criteria. Data included patients’ demographics (age, sex), comorbidities, limb involved (lower vs. upper), type of tumor, size, history of neo or adjuvant chemo and/ or radiation, and type of reconstruction. Wound complications were classified as minor or major.
Results: We reviewed 160 cases of upper and lower extremity sarcoma. 141 cases were closed primarily,18 closed with pedicle flaps and 1 with free tissue transfer. From the 141 primary closures, 54 needed to go back to the OR due to complications of which 22 required a pedicle flap, 8 required a free flap and 24 had a combination of washout +/- FTSG/STSG with or without wound vacuum with primary vs. secondary wound healing. 17 patients that were closed primarily received neo and adjuvant radiation therapy and 100% of these patients suffered wound complications requiring return to the OR. Wounds that were > 500 cm3 had a complication rate of 74% and wounds < 500 cm3 had a rate of 30%. The wounds that were secondarily reconstructed with a pedicle or free flap had no major complications whereas wounds that were primarily reconstructed with pedicle flap had a complication rate of 61%. In this series, the primary oncologic surgeon performed 81% of the primary flaps without the involvement of a plastic surgeon. The secondary pedicles vs. free flaps after the initial complications were done by plastic surgery, which had a secondary complication rate of 10 %.
Conclusion: Our data suggests that irradiated wounds and defects that are > 500 cm3, benefit from early involvement by a plastic surgeon. Early utilization of vascularized tissue, i.e. pedicle and free flap should be the first step in the reconstructive ladder for these high-risk patients. Early involvement of plastic surgery can have a significant impact on complication rates including re-operation and extended hospitalization.